Can we predict loneliness?
The loneliness epidemic has emerged as a widespread and debilitating issue, affecting thousands of individuals and contributing to poor mental health and related physical symptoms. This article explores whether it is possible to predict the risk of severe loneliness in individuals, enabling early intervention and support to those in need.
Project overview
This work explores the precursors of loneliness and investigates the potential to predict severe loneliness by analysing socio-economic and physical health factors. Although loneliness is not objectively measured, it is closely linked to various serious health and neurological disorders with physical implications.
Currently in its early stages, the project has identified correlations between loneliness and factors related to social structure and mental health, which could serve as the foundation for future agent-based modelling to map the incidence of loneliness and direct mental health resources as needed.
Data and methods
Loneliness is not a new phenomenon, but its widespread prevalence and debilitating effects have made it a major concern in recent years. This project, a collaboration between the Leeds University Business School (LUBS) and the School of Geography, University of Leeds, focuses on understanding the antecedents of loneliness and the correlations between loneliness and physical or psychological symptoms. Initially, the research was designed to make use of data from the Connected Yorkshire Research Database, which consists of anonymised electronic patient care data and self-reports of loneliness. However, due to challenges with accessing the data, the research pivoted to using data from the Understanding America Study (UAS).
As subset of the comprehensive UAS dataset spanning the period of the COVID-19 pandemic was used. It tracks the responses of over 8,300 survey participants longitudinally from March 2020 to January 2023 and includes more than 200,000 records and 4,000 variables. These variables cover a wide range of factors, such as income, retirement status, health conditions, and social behaviour. The key focus was on the frequency of a person experiencing loneliness, measured by asking participants, “How often have you felt lonely (days in a week)?” The research investigates correlations between loneliness and factors like economic deprivation, food insecurity, and chronic illness using statistical models, including chi-square tests and fixed effects models with loneliness as the response variable. This analysis was done using Python and statistical packages in STATA.
The study aims to track changes in the way respondents reported loneliness over time. Correlations between loneliness and other factors such as chronic illnesses, number of household members, income group, race and social media use were investigated using chi-square tests and Cramer’s V to measure the strength of these associations. Mixed effects models were applied to assess the impact of different factors on loneliness over time. The results showed that household income and marital status had a statistically significant effect on loneliness, while other factors, such as depression, which had previously shown correlation, were not significant in the fixed effects model. After performing a Hausman-Wu test to compare a fixed effects model with a random effects model, it was found that the fixed effects model was more suitable for the data.
As loneliness may not be immediately observable, lagged variables were created to capture the delayed impact of certain factors on loneliness. This approach is commonly used in econometric models to observe the effects of certain factors over prolonged periods of time.
The research is based in the United States, but the insights gained are expected to inform similar UK studies when the Connected Yorkshire data becomes available.
Key findings
The analysis revealed that household income and marital status were statistically significant predictors of loneliness over time, while mental health conditions like depression, previously thought to have a strong association, were not as significant in the fixed effects model.

Figure 1: Line charts illustrating the self-reported frequency of loneliness (days per week) for four randomly selected participants over the duration of the survey. The charts display fluctuations in responses, with one participant consistently reporting no loneliness (less than 1 day per week), while another participant reports loneliness 5-7 days a week at multiple points in time. The data reflects both stability and variability in loneliness experiences across different individuals over the course of the study.
Figure 1 visualises the changes in the response to the question “How often have you felt lonely (days in a week)?” over time for four participants. The data reveals diverse patterns of loneliness reporting, alongside noticeable inconsistencies in response timelines—some participants contributed frequently across survey waves, while others participated sporadically, leading to gaps in the data. Additionally, there appears to be reluctance among some individuals to report feelings of loneliness, which, combined with the absence of a standardised metric, presents a challenge in accurately measuring this complex emotional state.
The incidence of loneliness reported in the dataset was mapped across the United States using Tableau. Figure 2 depicts the normalised response to the question “How often have you felt lonely (days in a week)?” across the different states. The state of California recorded the highest number of survey participants, but the data was normalised to ensure equal representation across all states. Although most states reported fewer instances of loneliness, Figure 3 shows that Rhode Island, New Hampshire, and Vermont exhibited notably higher levels of severe loneliness compared to other states. The reason for this trend is not clear and is one of the limitations of this study. A contributing factor to this, is probably the granularity of the data.
The granularity is limited to the state level and the depictions in Figures 2 and 3 are a summary of the state’s responses, hence lacking sufficient detail to accurately reflect the incidence of loneliness within specific regions or communities across the states.

Figure 2: Visualisation of the normalised incidence of loneliness across the US. States such as Rhode Island, New Hampshire, and Vermont show higher levels of loneliness based on the responses to the question, "How often have you felt lonely (days in a week)?" while most of the states exhibit lower scores of loneliness. Normalisation of the data allows for equal representation across states, despite the varying number of participants per state. The green regions represent states with lower normalised levels of reported loneliness, while red regions highlight areas with more severe instances.
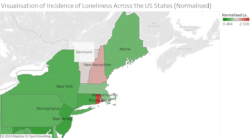
Figure 3: A zoomed in portion of the map in Figure 2 depicting the normalised incidence of loneliness in the northeastern states. Rhode Island, New Hampshire and Vermont show higher levels of loneliness, whereas many neighbouring states, including New York, Pennsylvania, and Massachusetts, report lower incidences.
Another key challenge in the study was the lack of discernible patterns in loneliness over time. The variable did not exhibit any significant change in relation to the associated factors likely due to weak correlations within the dataset. However, this could also be attributed to the limitations of the current data subset. Access to more granular and detailed NHS data, which is typically more factual and less subjective than survey-based responses, could potentially address these issues and provide deeper insights. A key issue here is that the NHS does not yet have a systematic method of recording loneliness in the form of a questionnaire or survey. Performing mental health surveys that record questions pertaining to loneliness could help unearth stronger associations between mental and physical health.
Value of the research
The loneliness epidemic is a growing issue with profound impacts on both mental and physical health. In the UK, an estimated 80% of respondents in the Community Life Survey reported experiencing varying degrees of loneliness, with approximately 4 million individuals frequently grappling with the debilitating effects of mental health disorders. Loneliness has been linked to a range of health complications, including depression, anxiety, Alzheimer’s disease, and even compromised immune function. Compounded by already strained mental health services, there is an urgent need to address this problem with innovative solutions.
The research offers significant value by identifying key factors contributing to severe loneliness, which can inform mental health policies and guide the allocation of resources. Policymakers and healthcare providers can use these insights to design targeted interventions that address both the socio-economic and health-related aspects of loneliness.
Moreover, by integrating these findings into future agent-based models, the spread of loneliness across populations can be simulated to predict high-risk areas and implement preventative measures before loneliness leads to more serious mental health conditions.
Insights
- Household income and marital status are strong predictors of loneliness over time.
- This study will be the basis of agent-based modelling studies to model the incidence of loneliness among people based on their physical health and socio-economic status.
- Data challenges (such as access to NHS data) highlight the importance of cross-country collaboration for further research and also highlights a lack of a metric to measure loneliness.
Research theme
Health & Societies
Programme theme
Statistical Data Science
People
Aditi Sudhakar, LIDA Data Scientist, University of Leeds
Dr Aulona Ulqinaku, Associate Professor of Marketing, Leeds University Business School, University of Leeds
Dr Jiaqi Ge, University Academic Fellow, School of Geography, University of Leeds
Partners
Leeds University Business School and Department of Geography, University of Leeds
Funders
Funded by the Consumer Data Research Centre (CDRC)